
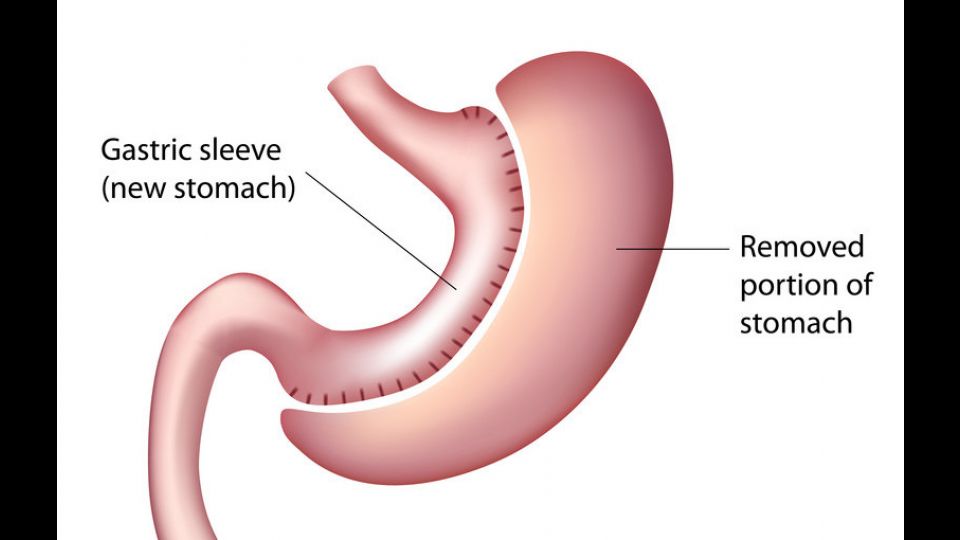
The intervention consists in removing 3/4 of the stomach, a tube through the mouth during the intervention in the stomach is used to calibrate the size of the new stomach. We cut it along the probe and at the same time the automatic clip sutures the section of the stomach. It thus poses a triple row of staples, but despite there is still a small risk of bad, or lack of healing on the installment of the section. There may thus appear a fistula with leakage of gastric contents in the ‘belly’, dreaded complication resulting re-intervention, drainage, put in place of prosthesis (see: Sleeve – Fistula – Complications).
- No complications after leaving the clinic, monitoring will be less systematic.
- Very important improval of diabetes, hypertension, sleep apnea.
- No vitamins' deficiency.
- The decrease in volume of the stomach will reduce the secretion of a hormone called ghrelin materializing the feeling of hunger.
- In second intention after failure of medical treatment, nutritional, dietary and psycho-therapeutic, well conducted during 6 to 12 months.
- In absence of sufficient weight loss or in absence of weight loss maintenance, diets supervised by a specialist (nutritionist, dietitian, endocrinologist…), with written proof (prescriptions etc…) very important for your medical insurance company !
- Patient well-informed in advance.
- Assessment and multidisciplinary preoperative support for several months.
- Procedure and need understood and accepted by the patient for life during medical and surgical follow-up.
- Acceptable operative risk.
Let’s emphasize once again that, whatever the chosen intervention, a life long change of dietary habits and lifestyle is essential. Bariatric surgery is no cosmetic surgery. Long term follow-up is necessary.